Massive ‘horse’ lies about Nobel prize winning treatment
09/25/2021 / By News Editors

STORY AT-A-GLANCE
- KFOR news ran a fake story in which a doctor claimed emergency rooms in Oklahoma were inundated with people who used horse ivermectin paste as a treatment for COVID-19 and overdosed
- The story turned out to be pure fiction, as no such cases have occurred. Still, KFOR has not retracted the story or issued a correction
- The idea that ivermectin is a horse dewormer that poses a lethal risk to humans is a deceptive narrative aimed at dissuading people from using a safe and effective drug against COVID-19
- While ivermectin is used as a dewormer in animals, it is also a human drug, approved by the FDA since the mid-1990s. It’s on the World Health Organization’s list of essential medicines for several parasitic diseases and, like many other drugs, ivermectin is used off-label for other diseases and conditions
- In addition to being antiparasitic, ivermectin also has potent antiviral properties and has even been shown to protect against SARS-CoV-2 spike protein damage
(Article by Dr. Joseph Mercola republished from Articles.Mercola.com)
In recent days, another big, fat lie has been allowed to circulate unchecked and unverified in headlines across the media landscape. “Ivermectin: Why Are U.S. Anti-Vaxxers Touting a Horse Dewormer as a Cure for COVID?” asks the Independent.1 Similar headlines — all focusing on “horse dewormer” — have been plastered across many other media outlets.
It appears Oklahoma’s KFOR news was the first to run a fake story that made this false narrative explode. September 1, 2021, KFOR reported that emergency rooms were overrun with patients who had overdosed on horse ivermectin. The claim was supposedly made by doctor Dr. Jason McElyea. According to KFOR:2
“Dr. McElyea said patients are packing his eastern and southeastern Oklahoma hospitals after taking ivermectin doses meant for a full-sized horse, because they believed false claims the horse de-wormer could fight COVID-19.’The ERs are so backed up that gunshot victims were having hard times getting to facilities where they can get definitive care and be treated,’ he said.”
Fake News Alert
Other media outlets ran with the story, including Rolling Stone magazine,3 The Daily Mail,4 the Independent,5 Newsweek,6 The Guardian,7 Yahoo News8 — which later published a story saying a hospital was “disputing” the claim — and MSNBC’s Rachael Madow.9
There was just one problem. It was a fake story. A few days after the story made major media rounds, the Sequoyah Northeastern Health System issued a public notice and posted it on its website homepage, dismissing McElyea’s claims as pure fiction:
However, rather than retract the article, which would be appropriate for a piece that turns out to be fictional from start to finish, Rolling Stone simply posted an “update” at the top of the article, noting Sequoyah’s rebuttal. KFOR has issued no correction at all, as of September 7, 2021. The Guardian issued an update at the bottom of its article, but did not include the hospital’s statement that NO patients have been treated for ivermectin overdose.
Hundreds of news articles have also brought attention to alleged rises in ivermectin-related calls to poison control centers around the U.S. These too, it turns out, are based on the flimsiest of data. For example, in Kentucky, poison control reports having received six calls relating to ivermectin paste overdose, compared to an average of one per year.
The department of health in Mississippi similarly noted that while calls to poison control involving ivermectin paste have seen a slight increase, all cases have been mild and none have required hospitalization due to toxicity.10 Clearly, people are not dying from horse ivermectin overdoses, and they’re certainly not dying from appropriately-dosed and prescribed oral ivermectin.
False Narrative Alert
This idea that ivermectin is a horse dewormer that poses a lethal risk to humans is pure horse manure, shoveled at us in an effort to dissuade people from using a safe and effective drug against COVID-19.
The intent is clear. What our so-called health agencies and the media are trying to do is confuse people into thinking of ivermectin as a “veterinary drug,” which simply isn’t true. Ultimately, what they’re trying to do is back up the Big Pharma narrative that the only thing at your disposal is the COVID shot. As noted in a recent HuffPost article:11
“Health experts ? the kind who practice on humans ? agree that the best way to prevent yourself from catching the virus is to get vaccinated, wear a face mask and stay out of crowds.”
In an August 21, 2021, Twitter post,12 the Food and Drug Administration said, “You are not a horse. You are not a cow. Seriously, y’all. Stop it,” linking to an FDA article on why you should not use ivermectin to prevent or treat COVID-19.
The MSNBC report in the video above is another perfect example of the deceptive narrative being spun around ivermectin. The host blatantly mixes data points together, talking about ivermectin horse paste in one breath and rising prescriptions for ivermectin in the other, as if doctors are now prescribing veterinary drugs just to appease desperate patients. He then goes on to refer to doctors’ success with ivermectin as “anecdotal.”
Comedian and podcast host Joe Rogan, who recently developed COVID-19 and treated it with ivermectin and a slew of other remedies, is also being badmouthed for daring to share his success story. NPR, for example, reported:13
“Joe Rogan has told his Instagram followers he has been taking ivermectin, a deworming veterinary drug formulated for use in cows and horses, to help fight the coronavirus. The Food and Drug Administration has warned against taking the medication, saying animal doses of the drug can cause nausea, vomiting and in some cases severe hepatitis.”
This video contains uncensored dialogue
Did Rogan take horse ivermectin paste? No. Did he take animal doses of it? No. As you can see in the video above, Rogan talked with “multiple doctors” who told him to take it and, ultimately, he did take it and he got well, remarkably quickly. Yet NPR blatantly blends veterinary and human use together, as if to insinuate that he did take horse-level doses of it.
It’s worth noting that the FDA is not warning against low-dose oral ivermectin as routinely prescribed for human use. They’re warning against animal doses, which no licensed medical doctor would prescribe. In short, doctors are not prescribing ivermectin for horses, nor are they prescribing it at horse dosages.
Ivermectin Is an Essential Human Drug
While ivermectin is used as a dewormer in animals, it is also a human drug, approved by the FDA since the mid-1990s for the treatment of river blindness.14 It’s also on the World Health Organization’s list of essential medicines for several parasitic diseases.15
Like many other drugs, ivermectin is also used off-label for other diseases and conditions. Systemic lupus and papulopustolar rosacea,16 for example, are sometimes treated with ivermectin. In 2018, a patent was filed to treat certain autoimmune disorders with ivermectin.17
When used preventatively for COVID-19, or as treatment for acute SARS-CoV-2 infection, ivermectin is being used off-label, but there’s nothing unusual or suspect about this at all. Many drugs are used “off label.” So, when media warn that “ivermectin is not approved by the FDA for the treatment of COVID-19,” that essentially means nothing. It certainly doesn’t mean the drug isn’t FDA approved at all, or that it’s only approved for animals.
The fact is, ivermectin has several different properties. In addition to being antiparasitic, it also has potent antiviral properties and has even been shown to protect against SARS-CoV-2 spike protein damage.
Research shows ivermectin impairs the spike protein’s ability to attach to the ACE2 receptor on human cell membranes.18 The drug can also help prevent blood clots by binding to SARS-CoV-2 spike protein. This prevents the spike protein from binding to CD147 on red blood cells and triggering clumping.19
As for safety, more than 4 billion doses have been given to (human) patients since 1998, and only 28 cases of serious adverse events have been reported in that time.20 Yet the FDA now claims ivermectin should not be used for COVID-19 because the drug may cause “serious harm,” is “highly toxic” and may cause “seizures,” “coma and even death”21 — warnings that are far more applicable to COVID shots.
Ivermectin Suitable for All Treatment Stages
Since early on, the Frontline COVID-19 Critical Care Alliance (FLCCC) has been trying to get the truth out about ivermectin. The FLCCC’s prophylaxis and early outpatient COVID-19 protocol is known as I-MASK+22 while the hospital treatment is called I-MATH+.23 All include ivermectin. As noted by the FLCCC in a news release:24
“The data shows the ability of the drug Ivermectin to prevent COVID-19, to keep those with early symptoms from progressing to the hyper-inflammatory phase of the disease, and even to help critically ill patients recover.
… numerous clinical studies — including peer-reviewed randomized controlled trials — showed large magnitude benefits of Ivermectin in prophylaxis, early treatment and also in late-stage disease. Taken together … dozens of clinical trials that have now emerged from around the world are substantial enough to reliably assess clinical efficacy.”
FLCCC president and chief medical officer Dr. Pierre Kory has testified to the benefits of ivermectin before a number of COVID-19 panels, including the Senate Committee on Homeland Security and Governmental Affairs in December 202025 and the National Institutes of Health COVID-19 Treatment Guidelines Panel in January 2021.26
The two protocols — I-MASK+27 and I-MATH+28 — are available for download on the FLCCC Alliance website in multiple languages. The clinical and scientific rationale for the I-MATH+ hospital protocol has also been peer-reviewed and was published in the Journal of Intensive Care Medicine29 in mid-December 2020.
Strong Evidence for Ivermectin
April 24 through 25, 2021, Dr. Tess Lawrie, director of Evidence-Based Medicine Consultancy Ltd.,30 hosted the first International Ivermectin for COVID Conference online.31
Twelve medical experts32 from around the world — including Kory — shared their knowledge, reviewing mechanism of action, protocols for prevention and treatment, including so-called long-hauler syndrome, research findings and real world data. All of the lectures, which were recorded via Zoom, can be viewed on Bird-Group.org.33
A one-page summary of the clinical trial evidence for ivermectin is available on the FLCCC website,34 while a listing of all ivermectin trials done to date, with links to the published studies, can be found on c19Ivermectin.com.35 So, what does the evidence show? In summary, studies have demonstrated ivermectin:36
- Lowers viral load.
- Inhibits replication of many viruses, including SARS-CoV-2 and seasonal influenza viruses. An observational study37 from Bangladesh, which looked at ivermectin as a pre-exposure prophylaxis for COVID-19 among health care workers, found only four of the 58 volunteers who took 12 mg of ivermectin once per month for four months developed mild COVID-19 symptoms, compared to 44 of the 60 health care workers who had declined the medication.
- Inhibits inflammation through several pathways and protects against organ damage.
- Prevents transmission of SARS-CoV-2 when taken before or after exposure.
- Speeds recovery and lowers risk of hospitalization and death in COVID-19 patients — The average reduction in mortality, based on 18 trials, is 75%.38 A WHO-sponsored review39 suggests ivermectin can reduce COVID-19 mortality by as much as 83%.
Who’s Actually Following the Science?
As noted in an August 3, 2021, review paper in New Microbes New Infections, titled “Ivermectin: A Multifaceted Drug of Nobel-Prize Honored Distinction With Indicated Efficacy Against a New Global Scourge, COVID-19”:40
“In 2015, the Nobel Committee for Physiology or Medicine, in its only award for treatments of infectious diseases since six decades prior, honored the discovery of ivermectin (IVM), a multifaceted drug deployed against some of the world’s most devastating tropical diseases.
Since March 2020, when IVM was first used against a new global scourge, COVID-19, more than 20 randomized clinical trials (RCTs) have tracked such inpatient and outpatient treatments. Six of seven meta-analyses of IVM treatment RCTs reporting in 2021 found notable reductions in COVID-19 fatalities, with a mean 31% relative risk of mortality vs. controls.
During mass IVM treatments in Peru, excess deaths fell by a mean of 74% over 30 days in its ten states with the most extensive treatments. Reductions in deaths correlated with the extent of IVM distributions in all 25 states with p < 0.002.
Sharp reductions in morbidity using IVM were also observed in two animal models, of SARS-CoV-2 and a related betacoronavirus. The indicated biological mechanism of IVM, competitive binding with SARS-CoV-2 spike protein, is likely non-epitope specific, possibly yielding full efficacy against emerging viral mutant strains.”
Despite the evidence, the American Medical Association (AMA), the American Pharmacists Association (APhA) and the American Society of Health-System Pharmacists (ASHP) are now banding together to call on doctors to immediately stop prescribing ivermectin for COVID outside of clinical trials.41
Hopefully, doctors will evaluate the evidence for themselves and do what makes sense and is best for their patients, rather than cater to Big Pharma. Indeed, as the U.S. wants to eliminate all use of ivermectin, other countries are starting to use more of it. India, for example, has added ivermectin for COVID-19 to its list of essential medicines.
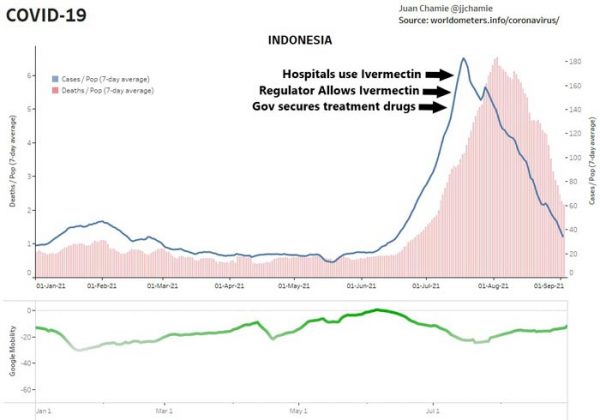
The Tokyo Metropolitan Medical Association also added ivermectin to its home treatment protocol August 13, 2021, and Indonesia’s government not only authorized the use of the drug but also created a website showing real-time availability of the drug. Hospitals in Indonesia started using ivermectin July 22, 2021. By the first week of August, cases and deaths were plummeting.42
The ‘Delta Variant’ Is Vaccine Injuries, Whistleblower Claims
In a recent Stew Peters program, a nurse blows the whistle on several commonly-held beliefs. She points out that her hospital was never, not even during the height of the pandemic 2020, over capacity due to COVID patients. Disturbingly, she notes that most hospital personnel are still unaware that the PCR test is completely unreliable, and care is all based on that test.
Even if you do not have any COVID symptoms, a positive test will land you on the COVID ward, where standard protocol calls for Remdesivir and, if you have low oxygen, being put on a ventilator. She says most patients get worse on Remdesivir, which has been shown to cause heart and kidney problems. She points out that for a short time, the drug was given in combination with ivermectin, and during that time, patient outcomes were much better. Ivermectin was then removed from the protocol.
As for the Delta variant, there are no commercial tests that will identify variants, although genetic sequencing in a research lab would be able to differentiate them. The nurse stresses that she’s never seen “Delta” specified on any patient chart — a claim that raises the question how officials are able to claim that most COVID-19 patients are now infected with the Delta variant.
She’s also reporting seeing a significant number of vaccine injuries, yet she’s not aware of a single instance where the injury was reported to the U.S. Vaccine Adverse Effect Reporting System (VAERS). Whenever she’s brought her suspicions to the doctor, she’s been rebuffed and the vaccine link has been dismissed.
The most shocking take-home from this interview is that the supposed surge in Delta cases are in fact mislabeled vaccine injuries, according to this whistleblower.
“The Delta variant is the vaccine injuries,” she tells Peters. “It’s common knowledge around the staff that is aware of what’s going on, [who are] paying attention [and] aren’t in denial.”
Read more at: Articles.Mercola.com
Tagged Under: Big Pharma, COVID, deception, Fact Check, fake news, hoax, ivermectin, lies, Media Lies, Medicine, pandemic, Prescription drugs, treatments
RECENT NEWS & ARTICLES